Strategically Rethinking HCP Engagement in 2026 & Beyond
- Karsten Schmidt

- Jan 5
- 6 min read
In Pharma, "Omnichannel" is everywhere, but often misunderstood, misapplied, or simply repackaged under new buzzwords. As companies are now planning for 2026, the challenge isn’t just more channels, it’s smarter engagement that reflects where each HCP is in their decision process. That's why we’re zooming in on Optichannel: a more targeted, outcome-driven approach that prioritises context over coverage.
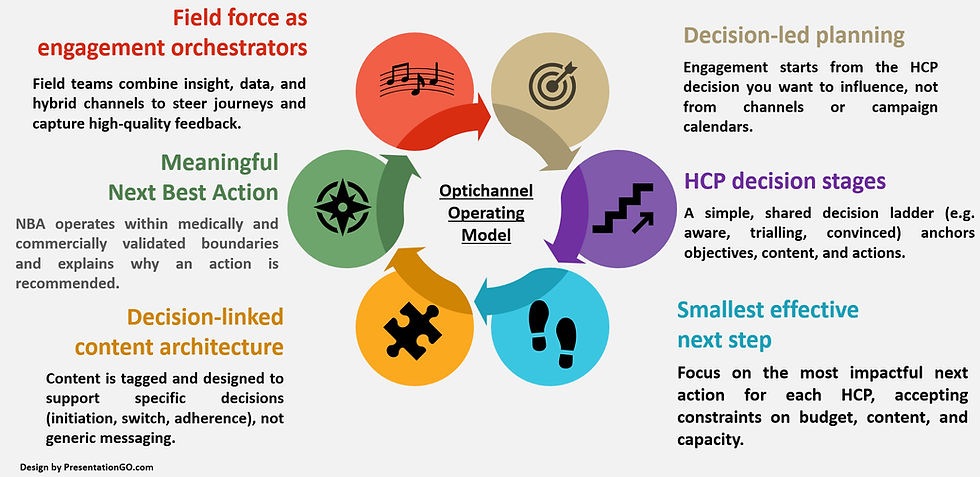
The illustration below summarises the core building blocks of an Optichannel operating model.
To unpack what this really means, and how to get it right, we spoke with Osman Daggezen, Founder of OD Pharma Consulting, whose deep expertise in Commercial Excellence, data strategy, and Omnichannel transformation brings clarity to a space filled with noise.
Karsten: Thank you for joining us today, Osman. Let’s start the interview with a big one: What is the biggest misconception pharma leaders still have about Omnichannel, and how does Optichannel fundamentally change the game?
Osman: Thank you for the invite, Karsten. The biggest misconception is that Omnichannel is about doing more. More channels, more campaigns, more content. Many leadership teams still equate progress with higher email volumes, more digital touchpoints, and larger content libraries, while the underlying engagement logic stays the same as ten years ago.
True Omnichannel is not a channel expansion program. It is an operating model that links three things in a disciplined way. The HCP decision you want to influence, the content that supports that decision and the mix of channels that can deliver this content efficiently. Optichannel takes this one step further. Instead of asking “What else can we push”, it asks “Given this specific HCP, at this specific stage, what is the smallest and most effective next step.”
This shifts the discussion from coverage to trade-offs. You accept constraints on budget, content and field capacity, and you design journeys that are both clinically relevant and operationally realistic. That is where the game really changes.
Karsten: How can organisations practically identify the HCP’s decision stage, and use it to guide engagement rather than defaulting to channel-based planning?
Osman: You do not need a perfect model to start. For each priority brand, define a simple decision ladder that reflects real practice. For example, unengaged, problem aware, treatment aware, trialling, convinced and advocate. Align this with Medical and Commercial so that everyone uses the same language.
Then, define observable proxies for each stage based on the data you actually have. This can include prescribing behaviour, event participation, questions raised in the field, preferred evidence formats or engagement with specific content themes. The key is to keep the classification simple enough that field teams trust it and can correct it.
Once you have a working view of decision stages, planning changes .objectives are no longer “send three emails and one webinar” but “move this segment from treatment aware to trialling within six months.” Content, channels and field actions are then selected as a package that serves that progression, not as isolated tactics.
Karsten: Many companies struggle with data quality and fragmentation. What are the minimum data foundations needed to make Optichannel work in the real world?
Osman: In many projects I see, teams waiting for the perfect data lake before they change anything. That is not necessary. Optichannel requires a few non-negotiable foundations rather than a fully mature ecosystem.
First, a reliable HCP identifier and consent status that is consistent across core systems. If you cannot confidently say “this is the same person” and “we are allowed to engage in this way,” everything else becomes fragile. Second, a basic but complete interaction history for Sales, email, events and key digital touchpoints. It does not have to be extremely granular, but it must be accurate and timely.
Third, a practical content tagging and taxonomy approach that links each asset to a decision purpose, such as initiation, switch, adherence or patient selection. Even a small, well governed taxonomy is more valuable than a complex one that nobody applies correctly. Once these three foundations are in place, you can gradually enrich with additional data sources rather than waiting for an ideal state.
Karsten: Next-Best-Action is everywhere yet often fails. What distinguishes a meaningful NBA system from one that only creates noise for field and medical teams?
Osman: Most NBA programmes fail because they start from what the algorithm can optimise, not from what the business is trying to change. If the logic is built only on click propensities or channel costs, it produces suggestions that may look intelligent on paper but do not match real conversations with HCPs. Field and Medical quickly lose trust, and the system becomes background noise.
A meaningful NBA system starts from a clear decision model. For each brand and segment, you define the critical decisions, preferred content modules and acceptable channel options. The algorithm then operates within these medically and commercially validated boundaries. It prioritises across brands, applies frequency and relevance rules and explains why a certain suggestion is being made.
Equally important is the human loop. Field and Medical teams must be able to accept, adapt or reject suggestions and feedback on what actually happened. Their input should train the system over time. When they see that NBA removes administrative burden, supports better preparation and leads to more relevant discussions rather than more tasks, adoption follows naturally.
Karsten: How should the role of field force evolve in an Optichannel model, and which behaviours or capabilities will matter most in the next 2–3 years?
Osman: In an Optichannel model, field teams move from being primarily visit deliverers to becoming orchestrators of HCP engagement. Their value is not only in the number of calls they make, but in how they use every interaction to understand where the HCP is in the decision process and to shape the next step across channels.
Three behaviours stand out. First, preparation that combines clinical insight with data, such as understanding recent engagements, content preferences and questions raised by the HCP. Second, disciplined documentation of visit insights in a structured way, so that Medical, Marketing and NBA engines can use them. Third, comfort with hybrid engagement, where digital follow up, remote meetings and collaboration with Medical are part of the normal rhythm.
On the capability side, basic data literacy and curiosity will be critical. Field colleagues do not need to become data scientists, but they do need to understand how their inputs influence targeting, NBA and content planning. Organisations that invest in this mindset and align incentives with quality of engagement rather than single metrics such as call volume, will move faster.
Karsten: Which KPIs truly reflect decision progression across the customer journey, and which commonly used metrics should pharma start de-emphasising?
Osman: KPIs that matter in an Optichannel world describe whether HCPs are moving through the decision ladder and whether your engagement is helping or hindering that movement. Examples include the proportion of targets with a defined journey and decision stage, the percentage of HCPs progressing from one stage to the next within a given period and time to progression for priority segments.
You can complement this with decision linked engagement metrics. For instance, completion of specific learning paths before adoption, use of HCP selection tools, or follow through on agreed next steps after key interactions. These indicators tell you whether your content and channels are doing the job they were designed to do.
Metrics that deserve less weight on their own include raw email volumes, open rates without context, website visits without a clear next step and isolated call counts. They are still useful as operational indicators, but they should sit under a hierarchy that is anchored in decision outcomes. Otherwise, teams optimise the wrong things and still wonder why prescribing behaviour does not change.
Karsten: If you were advising leadership teams for 2026 planning, what one priority would you recommend to accelerate customer engagement transformation?
Osman: I would ask every leadership team to pick one priority brand and build a full decision led engagement blueprint for it, from top to bottom. That blueprint should define the HCP decision ladder, the key segments, the core journeys, the content architecture, the operating model between Sales, Medical and Marketing and a small but sharp KPI set.
Then, commit to running this as a real pilot throughout the year with proper governance and learning loops, rather than adding it as another slide in a strategy deck. Use this brand to test how NBA should work, how data should flow, how content should be tagged and how teams should collaborate. Document what works, what does not and why.
Once you have that concrete, lived example, scaling to other brands becomes much faster and more credible. It is this kind of focused, execution-oriented priority that turns Omnichannel and Optichannel from concepts into an everyday way of working.
Karsten: Thank you, Osman for sharing such clear, experience-driven perspectives. What stands out is the strong practical focus—moving beyond theory and tools toward decision-led engagement that works in real organisational settings. For leaders planning 2026 and beyond, this kind of realism is exactly what helps turn strategy into execution.
Omnichannel only creates value when decisions, content, and engagement logic are tightly aligned rather than expanded for the sake of coverage. Optichannel sharpens this further by focusing on the smallest effective next step for each HCP, using decision stages as the primary planning anchor instead of channel plans or campaign calendars. In this model, Next Best Action and field force impact are driven by clinical relevance and decision progress, with success measured by movement along the decision journey rather than isolated activity metrics.
As you look ahead to your 2026 planning cycle and beyond, where do you see the biggest gap today: understanding HCP decision stages, translating insights into action, or letting go of activity driven KPIs?



Comments